
Supporting Clinical Decision Making
The information on this page is also available here as a downloadable PDF, including links.
Current modelling suggests that COVID-19 will continue to affect critical care at least for the winter of 2020. In circumstances of stretched resources, where clinicians are balancing complex clinical situations, and when families may be restricted from or unable to attend hospital, clear and robust decision-making practices are essential. Patients may potentially deteriorate quickly, and early decisions will need to be made about what treatments they would both desire and benefit from, and in which setting they would best be cared for as outlined in NICE COVID-19 rapid guideline: Critical Care in Adults NG159.
This guidance is intended to bring together resources to support clinicians who are making decisions about care and treatment, and who are having conversations with patients and families in these difficult situations. The guidance is focussed on the following areas:
Making decisions around escalation of treatment
Involving others in decision-making
Supporting good communication with patients and their families
The guidance involves links to resources which may help, and you can adapt for local use. They are not new and have been widely used in the NHS.
Making decisions around escalation of treatment
Making difficult decisions surrounding clinical care is not a new problem, it is a daily experience for patients, families and doctors every day in the NHS. The process of shared decision making with patients and families is a part of Good Medical Practice as defined by the GMC. For patients lacking mental capacity these discussions are an integral part of determination of best interests, as outlined in the Mental Capacity Act. In order to ensure fair access to intensive care during the COVID-19 pandemic, it is recommended that a structured approach should be used when making such decisions.
Decisions to escalate, limit or withdraw life-sustaining treatments are the most relevant and the most ethically and emotionally charged and therefore require particular care. However, each decision should not be seen in isolation, but as a series of interdependent decisions in a patients' care. An important principle of clinical decision-making is that treatment decisions must always be based on a patient’s wishes, or in the individual patient’s best interests if lacking capacity, While this can be perceived as a binary choice between life-sustaining treatment or palliative care the reality is often more nuanced and complex, with multiple options available. Decisions must therefore be made after as full an exploration of the issues and context as possible. The resources highlighted here seek to achieve this goal.
While the contexts for treatment decision-making may be different, the following outline structure and resources below should help support both the clinician and patient in decision making:
Ensure you have a shared understanding between the clinicians, patient, and those close to the patient of what the problems and issues are.
Discuss what the likely outcomes are. Try to help the patient identify which outcomes are most important to them and their family.
Be clear about what treatments are being proposed. If a treatment is not considered sufficiently beneficial to be offered, this will need communicating carefully and compassionately.
Agree the proposed treatment plan and care you will be organising, for example treatment on the wardor treatment on intensive care.
Include discussion of specific treatments both that require discussion e.g. CPR, or are important to the patient.
Following the discussion, ensure that decisions, including CPR, are documented in an easily recognised format (e.g. ReSPECT, TEP, DNACPR plus ACP). This will help guide your fellow clinicians in an emergency situation, and some patients may already have such decisions documented which you should take account of.
Involving others
The conversation above assumes a patient with capacity to be involved in the decisions made. Where the patient lacks capacity, the clinician must try to contact those close to them, where practicable and appropriate, in order to find out about the patients’ values and beliefs to make a best interests decision If the patient has a lasting power of attorney for Health and Wellbeing then that attorney is legally empowered to make decisions on the patient’s behalf.
Professional guidance recommends important best interests decisions (e.g. ICU admission, withdrawal of life sustaining therapies) should be shared between at least two senior clinicians. This may not always be possible at times of extreme clinical pressure, particularly outside the intensive care environment. Mechanisms to ensure this can be achieved should be considered by individual organisations.
Decision Making Frameworks
These frameworks, tools and templates can all be adapted by teams to suit their population, workforce, and the changing circumstances. We will be adding best practice examples and further resources as they are developed and become available.
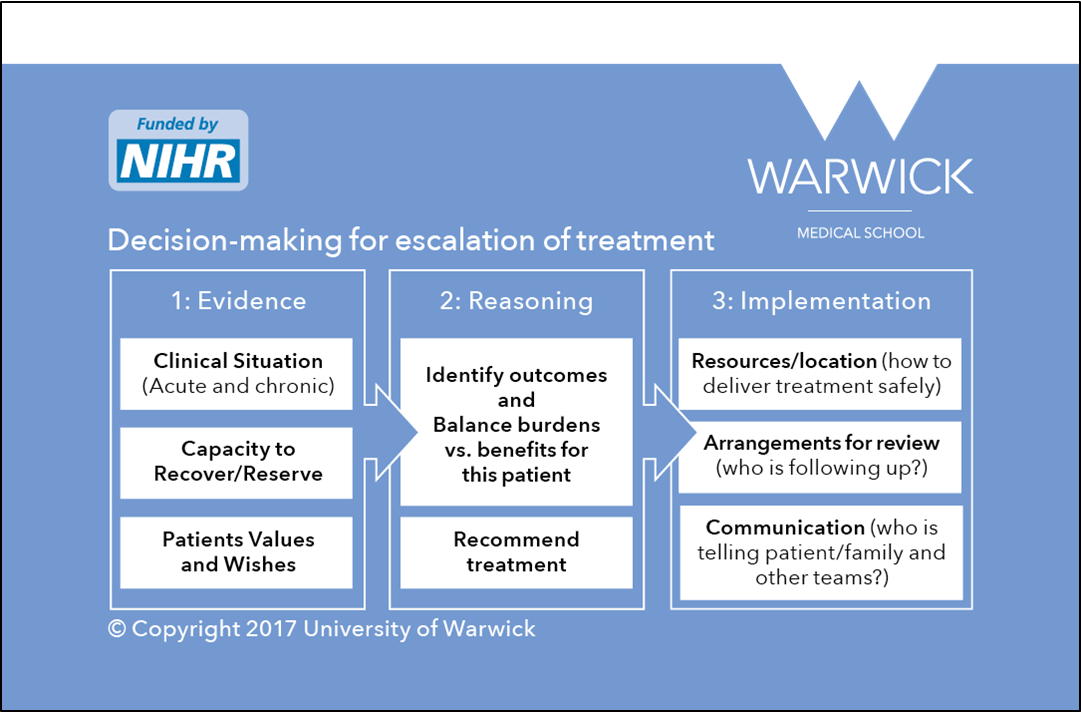
This model was developed by the University of Warwick from an observation of best and real-life practice in decision-making for escalation of treatment and admission to ICU. This model draws on the ethical framework of accountability for reasonableness. It focuses on gathering the right information about the particular situation to inform reasoning and to recommend treatment. It also guides the implementation, communication and on-going review of the patient. A review of the implementation showed that this introducing this model was feasible, promoted patient and family involvement, promoted patient centred decision-making, and the documentation of the rationale for decisions and transparency. It is recommended in the FICM end-of life guidance.
Resources are available in the following links and can be adapted for local use:
1. Summaries and a full report of this project are available from the National Institute for Health Research. Other resources are available from the University of Warwick project webpage.
2. A digital learning module based on the Warwick Model is available, is available on the E-LfH platform.
2. Decision-making structure: credit card reminder.
{kind=link}
3. Decision-making documentation
a. Referral form (information from referrers to help choose best treatment)
b) Decision-form (documentation to guide and document escalation decision).
MORAL Balance
An ethical framework to support bedside decision making, based on the four pillars of medical ethics, and designed to help clinicians apply them rapidly. Developed as part of NHS Blood and Transplant’s Deceased Donation Course for ICM trainees, but applicable widely. The framework has been taught to more than 300 ICM trainees over five years, and recommended in the FICM’s Care at the End of Life guidelines.
BJA Education Article describing framework & application
BJA Education Podcast, further discussion of application
Website - www.moralbalance.org inc. framework, video lectures and case examples
Documentation template - to help application and documentation
Supporting good communication with patients and their families
Clinicians will have conversations with patients in multiple settings, primary care, virtual clinics and during acute admissions. Isolation and illness may mean the patient is without their family, for support and to help advocate their wishes if capacity is lost. Clinical teams may need to use telephone/electronic communication, recognising the conflicts with confidentiality. Organisations should develop local policy for telephone conversations.
We have suggested some short resources to support good communication practice:
Intensive Care Society guidance on use of video communication
King’s Health Partners Lifelines project for virtual family visiting
Supporting pre-emptive decision-making outside ICU
During the COVID 19 emergency it will be necessary to build confidence and capability in doctors with a wide range of expertise and experience to share decision making. Opportunities should not be missed to gather information and make decisions when patients are able to participate in the process. Patients may deteriorate quickly, and decisions made in an emergency situation can be considerably more difficult. These resources are designed to help teams deliver this:
The ReSPECT ( Recommended Summary Plan for Emergency Care and Treatment) process is an excellent example of a TEP (Treatment Escalation Plan), of which there are several examples in use nationally. ReSPECT has been developed based on best evidence of how to support conversations and make sure that patients get the treatment that they want and would benefit from. It has been developed with input from clinicians from many different specialties, patient groups and others,and the support of the Resuscitation Council UK.
The ReSPECT process creates personalised recommendations for a person’s clinical care and treatment in a future emergency in which they are unable to make or express choices. These recommendations are created through conversations between a person, their families, and their health and care professionals to understand what matters to them and what is realistic in terms of their care and treatment.
ReSPECT is designed to be able to cross care settings, supporting decision making in primary care, and in ward and critical care environments.
References
Rees S, Bassford C, Dale J, Fritz Z, Griffiths F, Parsons H, Perkins GD, Slowther A-M, Implementing an intervention to improve decision making around referral and admission to intensive care: Results of feasibility testing in three NHS hospitals. Journal of Evaluation in Clinical Practice; February 2020: 26(1) 56-65.
F. Griffiths M. Svantesson C. Bassford J. Dale C. Blake A. McCreedy A‐M. Slowther. Decision‐making around admission to intensive care in the UK pre‐COVID‐19: a multicentre ethnographic study. Anaesthesia. November 2020. https://doi.org/10.1111/anae.15272.
Bassford C, Griffiths F, Svantesson M, Ryan M, Krucien N, Dale J, et al. Developing an intervention around referral and admissions to intensive care: a mixed-methods study. Health Serv Deliv Res 2019;7(39).
Harvey DJR, Gardiner D. `MORAL balance' decision-making in critical care. BJA Education. British Journal of Anaesthesia; 2019 Mar 1;19(3):68–73.